



The present study was conducted qualitatively and with a “grounded theory” approach, assuming that the concepts of ethical challenges are not known in pediatric physicians. The aim of this study was to explain the nature, structure, and process of formation of ethical challenges in pediatrics and to present a theory about how behaviors related to ethical challenges are formed.
According to Strauss and Corbin, a qualitative researcher must know how participants experience a phenomenon and what they understand about their experience. They always pay attention to the fact that explaining a phenomenon and describing the process of human actions, interactions, and emotions that occur in response to it is not comprehensive enough without considering the context and context of their formation [9]. The purpose of its implementation is, rather than describing a specific phenomenon, to develop a theory about the dominant social processes underlying the formation of that phenomenon [10]. Using this approach, researchers are able to examine social processes and explain the process of formation of a phenomenon, in the real conditions of its occurrence [11].
In the present study, considering the multifactorial nature of ethical challenges and the influence of various educational, economic, social and cultural factors on its occurrence, the “context-based theory” approach was chosen to explain the process and recognize the different dimensions of this phenomenon in pediatrics.
The researcher, after obtaining ethical approval, began sampling from available participants. informed consent was obtained from all the participants in the interview. Regarding the recording of the interviewee’s voice, Verbal informed consent was obtained. The research was conducted in accordance with the Declaration of Helsinki and other relevant national guidelines. After explaining the objectives, study methods, and ensuring the confidentiality of information, semi-structured interviews were conducted. Prior to each interview, a demographic information questionnaire was completed by participants (Table 1). Then, based on the interview guide, questions with the following concepts were asked: What ethical challenges have you encountered during clinical practice in children? What are your clinical experiences in this field? What solutions do you think of?
Then, based on the answers provided, the researcher guided the discussion to achieve the desired responses. The interviews with parents began with the question, “Does your child’s doctor involve you in the treatment process?” This question indicates the extent of family participation in the child’s clinical decision-making and the importance given to family requests. This open question provided a suitable basis for continuing the discussions. During the interviews, notes were taken about the participants’ nonverbal messages. The duration of the interview varied from at least 45 min to 2 h.
The questionnaire included general questions. Therefore, the information obtained from the participant determined the type of questions for the next interviewee. In this type of interview, the interviewee was asked to elaborate on the answers with the questions “Why? How? Explain more?”
Discovering and explaining the underlying psychosocial process of the data plays a very important role in integrating the data and forming the final theory. In a grounded theory study, the explanation of a psychosocial process is based on a theory that is formed around a central category. Therefore, the questions were about reasons, contexts, possibilities, consequences, diversity, and conditions, which helped the researcher in extracting theoretical codes. The information was collected through in-depth individual interviews, observation methods, and note-taking of nonverbal messages. Interviews were conducted with the agreement between the researcher and the participant, in line with scientific interview principles, and were subject to change. To ensure maximum diversity, samples were selected from general practitioners in Tehran city or healthcare centers, specialized and subspecialist pediatricians with private practices or full-time university faculty members in Tehran, nurses working in educational hospitals, and parents of sick children with various socio-economic backgrounds in different government, educational, and private hospitals.
A total of 39 interviews were conducted (21 physicians, 15 parents, 3 nurses). The analyst continuously gathered, coded, and analyzed data to develop the emerging theory during the process. The researcher decided which data to collect at each research stage and which group of physicians to select as the next sample. Selection of individuals, groups, or other sampling considerations was based on the evolving theory, aiming to create a new level of insight that would support the developing theory. Subsequently, the research progressed based on theoretical sampling. In this type of sampling, the selection of each sample was carried out after initial interviews and the emergence of initial classifications. The selection of interviews included available pediatricians, general practitioners, nurses working in hospitals, and parents of sick children from different socio-economic backgrounds selected from various government-teaching and private hospitals. After completing each interview, interview transcripts and data analysis, initial (free) coding was performed, and based on the concepts derived from the categories, the researcher decided which group of physicians to select for the next interview. The study continued based on theoretical sampling. The duration of data collection for this study was from July 2014 to March 2015 and was analyzed simultaneously.
During the open coding phase of this study, after each interview, the audio file was listened to and transcribed word for word and must be analyzed before conducting the next interview. This way, each interview directed the subsequent one. Following the transcription of each interview, the audio files were reviewed again, and notes were taken regarding key points made by participants, as well as the researcher’s thoughts and interpretations of their statements, in the margins of the transcripts. Data analysis was done using a line-by-line analysis method. The transcribed texts of each interview were read multiple times, key sections were highlighted using Word software, and conceptual codes or direct quotes reflecting what participants had said were identified. The coded versions were reviewed after a few days, recoded, and compared for consistency. The results of the two coding phases were compared to ensure code consistency, data stability, and alignment. Some of the coded excerpts were shared with participants for validation, and their acceptance was confirmed. In the axial coding phase, the analyst systematically formed categories, established relationships between them and subcategories. Similar meaningful codes were grouped together in this phase to form the broadest categorization first, followed by the inclusion of subcategories in subsequent stages. After axial coding, the researcher engaged in an iterative process of breaking down, comparing, and re-categorizing, aiming to refine, complete, and develop the categories. New categories with explicit names and concepts were identified and formed as subcategories. Subsequently, in the selective coding phase of the current research, the categories were linked together to develop a theory explaining ethical challenges in pediatric medicine. The researcher continuously reviewed initial data, notes, and conducted comparative analyses to harmonize and discover relationships between primary and subcategories, refining and developing theoretical concepts and codes. These actions enabled the researcher to integrate the concepts obtained during open and axial coding stages, using them to select a central category. The researcher then proceeded with theoretical coding, aiming to transition from descriptive statements to theoretical statements and abstract thinking. All possibilities influencing the data analysis process and findings were carefully considered to move towards theoretical and abstract formulations.
In the stage of explaining the core codes based on the content of each category, which included subcategories based on common characteristics and dimensions,
A total of 22 main categories and 8 subcategories were formed, which were the result of repeated movement between different categories and concepts.
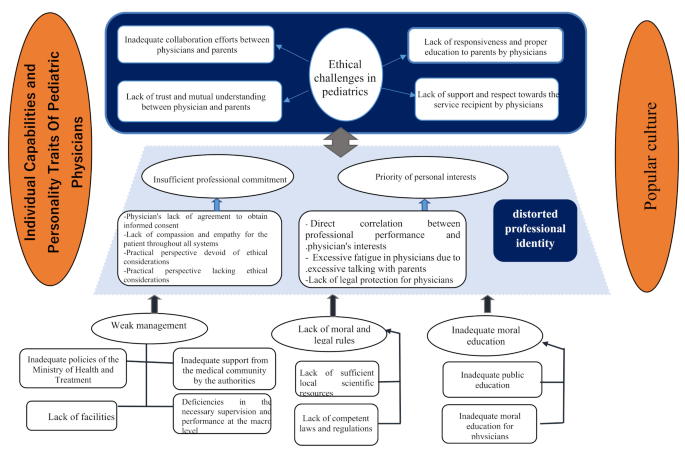
In this section, the process of forming ethical challenges in pediatric physicians was described in the form of seven conceptual categories: “ethical challenges”, “distorted professional identity”, “management weakness”, “legal ethical vacuum”, “common culture”, “ineffective medical ethics education”, “individual competence and personality traits of the pediatrician”, and their relationship structure with each other and with the central category was explained.(Table 2).
Discovering and explaining the basic psychosocial process of the data plays a very important role in integrating the data and forming the final theory. Explaining the basic psychosocial process is based on a theory that is formed around the central category. Questions that can help the researcher in extracting theoretical codes include: What is the cause of these behaviors? Under what circumstances do they occur? What are their results? In general, the question will be about reasons, contexts, possibilities, consequences, diversity, and conditions.
At this stage, the central code titled “Ethical Challenges” that was explained in the process of analysis and comparison among conceptual classes, indicated the existence of clinical ethics problems in the field of doctor-patient interaction in pediatrics.
These concepts include: (1) Insufficient cooperation of the doctor with parents and child (2) Lack of support and respect for the service recipient by the doctor (3) Lack of trust and mutual understanding between the doctor and parents (4) Lack of appropriate accountability and education to parents by the doctor.
By using these behavioral patterns with the service recipient, doctors have created ethical challenges in pediatric clinics. Which leads to the creation of undesirable relationships between the doctor and the patient child and parents and causes dissatisfaction.
Based on the analysis of the concepts explained in the categories and axial codes, the factors that lead to the formation of ethical challenges in the pediatric clinic were obtained. In designing the pattern of the formation of ethical challenges, the axial code of compromised professional identity was selected as the central code, and the other explained axial codes lead to the formation of a distorted professional identity for the pediatrician, and the operational result of this identity leads to the creation of explained ethical challenges in the pediatric clinic (figure 1).

Ethical issues in Iranian pediatrics
link