

Characteristics of the sample
A total of 838 (46.6%) out of 1800 invited participants completed both the demographic questionnaire and the open-ended questions. Most participants were female (97.4%, n = 816), and the main workplace was medical wards (38.5%, n = 323). Very few (15.0%, n = 126) participants reported receiving ACP training. Table 1 contains further information on the demographic and professional characteristics of the participants. From the analysis, three categories and six themes emerged from the data. Table 2 shows the ethical challenges identified by nurses. Fig. 1 reveals a coding tree illustrating the hierarchical relationship between categories, themes, and codes.
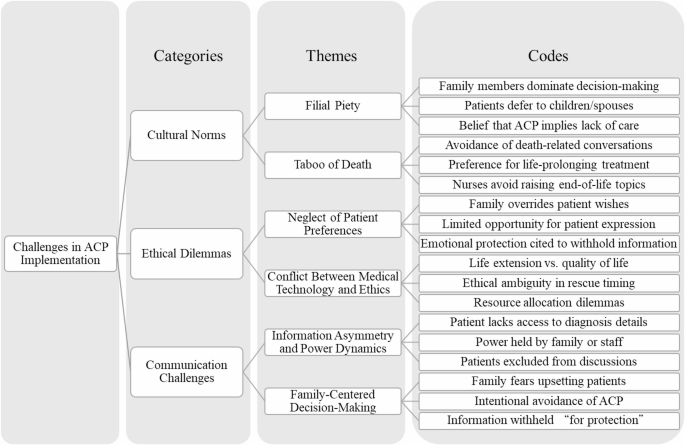
Coding tree of categories, themes, and codes
Cultural norms influencing implementation
The finding revealed that cultural factors, particularly “filial piety”, significantly influenced ACP decisions. Among all open-ended responses, 15.6% (n = 291) mentioned filial piety as a key influencing factor in decision-making. The traditional concept of filial piety often led families to dominate medical decision-making, thereby limiting patient autonomy. Specifically, 141 responses mentioned that “families (children) were reluctant to discuss these issues with the patient”, reflecting a deep-rooted belief in the duty to provide all possible care. Some responses (n = 38) suggested that initiating ACP discussions implied a failure to provide adequate care. This belief further led to 73 responses mentioning that “patients were often unaware of their true medical condition”, as families believed that protecting patients from the “shock” of their illness was a sign of filial piety. Additionally, N325 response indicated that “patients often delegated medical decision-making to their families (such as spouses or children), prioritizing family harmony over personal involvement.”
The “taboo of death” emerged as another significant cultural barrier to ACP decision-making. The responses revealed a widespread avoidance of death-related discussions among families (n = 62), with a prevalent preference for life-prolonging treatments (n = 56). This behavioral pattern reflects a cultural sensitivity and avoidance of death-related topics rather than being solely based on the patient’s actual preferences. Furthermore, 23 responses indicated that nursing professionals themselves were influenced by the “taboo of death,” avoiding initiating discussions about death-related issues. This phenomenon may be attributed to the permeation of cultural norms into professional practices or may reflect deficiencies in nursing professionals’ communication skills or institutional support. Notably, the “taboo of death” was not merely about avoiding discussions; it also manifested as a strong belief in the sanctity of life. N129 response mentioned the Chinese saying “it’s better to live a miserable life than to die,” reflecting a cultural belief that prioritized life preservation, even at the expense of quality of life. Consequently, families were more inclined to opt for aggressive treatments rather than pursuing palliative care options that might align more closely with the patient’s true wishes.
Ethical dilemmas in decision-making
A significant ethical dilemma in decision-making is the “neglect of patient preferences.” Responses indicated that healthcare teams and families often prioritize aggressive medical interventions over the patient’s expressed wishes. As stated in 32 responses, families were “reluctant to discuss these issues with the patient,” resulting in the patient’s voice being marginalized in decision-making. Additionally, 3 responses highlighted that even at the end of life, families often pursued “aggressive life-prolonging measures,” indicating a strong desire to prolong life that often superseded the patient’s actual wishes. Furthermore, patients’ ability or opportunity to express their preferences was limited, as evidenced by 18 responses indicating that patients were unable to articulate their preferences due to their medical condition, cultural background, or lack of information.
Another significant ethical dilemma is the “conflict between medical technology and ethics.” Respondents highlighted the critical challenges healthcare teams encounter when navigating end-of-life medical interventions, particularly the complex decision-making processes surrounding “uncertain rescue timing” and “appropriate moments for patient-family discussions”. This inherent uncertainty underscores the ambiguous boundaries between technological application and ethical deliberation in clinical practice. Specifically, seven responses critically examined whether “medical interventions genuinely respect patient quality of life”, emphasizing potential ethical dilemmas arising from excessive technological dependency. Moreover, three responses addressed “end-of-life medical resource allocation”, illuminating the profound ethical considerations required when deploying technological capabilities to make resource utilization decisions.
Practical challenges in patient-provider communication
A significant practical challenge in patient-provider communication is the “information asymmetry and power dynamics”. As indicated by 26 responses, the authoritative stance of nursing professionals often limits patients’ and their families’ access to information. This power dynamic not only undermines patients’ right to know but also weakens their proactive involvement in decision-making. The direct consequence of such information asymmetry is evident in 58 responses highlighting patients’ “insufficient understanding of their own medical condition,” and N525 even replies: “Some Times, doctors only talk to the family in a separate room; we are not even invited.” This may be attributed to inadequate information provision by nursing professionals or deliberate concealment by families. Furthermore, 42 responses mentioned “poor communication among physicians, nurses, patients, and families,” indicating a breakdown in multi-party communication that exacerbates information asymmetry. Additionally, 16 responses pointed out the “inability of nursing professionals to communicate with patients in a timely and appropriate manner,” suggesting a reliance on unidirectional information transmission rather than interactive and transparent communication.
The “family-centered decision-making” (33.1% of codes) further complicated boundary ethics in nursing practice, as nurses had to navigate conflicting expectations.179 mentioned “fearing that discussing the situation would upset the patient,” while 106 noted families were hesitant to discuss sensitive topics to avoid “burdening the patient.” Furthermore, 86 responses mentioned that “families were reluctant to discuss these issues with the patient,” often motivated by a desire to “protect” by withholding information or minimizing discussions. This protective behavior sometimes extended to information control, as seen in 29 responses where families explicitly stated that they “did not want the patient to know about their cancer diagnosis.” This highlights the systemic issue of power imbalances in ACP discussions, where patients’ voices are often marginalized.
A conceptual model of cultural norms, ethical dilemmas, and communication challenges in ACP
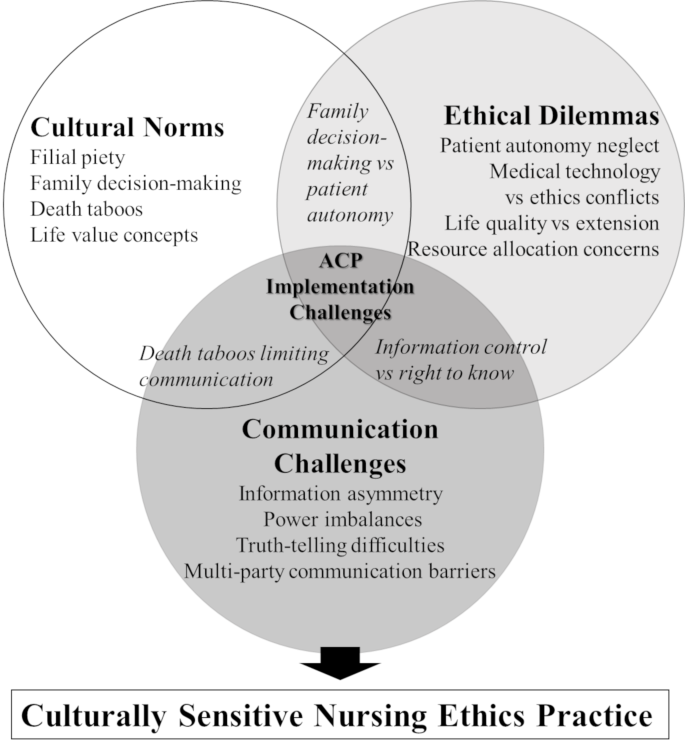
The thematic analysis of nurse responses revealed a dynamic interplay among cultural norms, ethical dilemmas, and communication challenges in the implementation of ACP within the Chinese healthcare context (Fig. 2). This figure illustrates the interaction and overlaps of these three domains, generating specific implementation challenges at their intersections.
The cultural norms domain encompasses two primary themes: filial piety and death-related taboos. These deeply ingrained cultural values significantly influence attitudes towards end-of-life discussions among families and healthcare professionals. The ethical dilemmas domain highlights two core challenges: the disregard for patient preferences and the conflict between medical technology and ethical principles. The communication challenges domain focuses on information asymmetry, power dynamics, and family-centered decision-making, all of which complicate transparent communication.
Furthermore, based on participant responses, the researchers identified key areas where these domains intersect. At the intersection of cultural norms and ethical dilemmas, the tension between familial decision-making authority and patient autonomy is paramount. When cultural norms meet communication challenges, death-related taboos pose significant barriers to open dialogue. Between ethical dilemmas and communication challenges, information control practices conflict with patients’ rights to understand their medical condition.
At the core of this dynamic interaction diagram lies the convergence of all three domains, representing the central challenge for nurses implementing ACP in the Chinese context: developing culturally sensitive ethical nursing practices that balance respect for traditional values with the protection of patient rights. This conceptual framework provides a foundation for developing targeted interventions that address these specific intersections, rather than treating each challenge in isolation.
link





