

A mixed methods approach was used, employing a sequential exploratory design. In the initial phase, interviews were conducted with 20 healthcare professionals to identify and analyze key themes using conventional content analysis. The second phase involved developing and refining a 50-item questionnaire with input from a panel of 15 experts. This questionnaire was pretested with 30 healthcare professionals. Subsequently, a shorter 30-item questionnaire was created, utilizing a five-point Likert scale, and tested with a larger sample of 300 healthcare professionals. The psychometric properties of the questionnaire were assessed through factor analysis and reliability testing.
Phase I. Instrument development
Qualitative study
In this phase of the present study, the researchers aimed to define and explain the concept of moral intelligence in the cardiac operating room from the perspective of healthcare professionals. To achieve this, they utilized the qualitative content analysis method. Because qualitative content analysis research can help explain a phenomenon in the cultural context of people’s perspectives who deal with a phenomenon for a long time27. Conventional content analysis is one of the most common and important qualitative content analysis methods. It allows for a better understanding of how individuals perceive and make sense of a phenomenon by identifying both commonalities and differences in their interpretations28. Also, conventional qualitative content analysis is an appropriate procedure for obtaining reliable and valid results from textual data, allowing the creation of new knowledge and innovative understanding of phenomena under investigation29. Therefore, a qualitative approach with conventional content analysis has been used to investigate this subject.
Twenty healthcare professionals from cardiac operating rooms in two public centers affiliated with medical universities in Iran’s west and southeast regions were selected with purposeful sampling. The criteria for inclusion were being willing to participate, having at least 12 months of work experience in the cardiac operating room, being Iranian, and having a good command of Farsi.
The study utilized various methods for data collection, including face-to-face, semi-structured interviews, observation, and field notes. A total of 20 healthcare professionals were interviewed in quiet hospital settings, when the participants did not have a shift. The time and location of the interviews were selected based on the participants’ preferences. Additionally, participants were asked to permit us to observe their performance for one working day during each interview. All participants agreed to allow us to observe their performance in the operating room for one working day. As a result, data for this study were collected through semi-structured interviews and observations of 20 professional healthcare workers.
The interviews were thorough and aimed to understand the participants’ perspectives better. Each interview began with a few general questions, including” “Can you describe a day of your working in the cardiac operating room”? and” What do you think competence means for health care professionals in the cardiac operating room?”, “What factors affect the competence of the personnel in the cardiac operating room?” “What does moral intelligence mean to you?” “In your opinion, what factors are effective in the moral intelligence of personnel in the cardiac operating room?”. Subsequently, based on the ’respondents’ answers, follow-up questions would be asked to increase the clarity of the information—the questions included, “Can you explain further?”, “What do you mean by that?” and “Can you give an example?”. Based on the participant’s answers, other questions were asked to probe other aspects of moral intelligence further. The interviews were audio-recorded, observation and field notes were taken with the permission and awareness of the participants. Each interview lasted between 50 and 70 min. Immediately after conducting each interview, the first author listened to the recordings multiple times to gain a comprehensive understanding and to identify the key insights. This initial analysis was conducted following each interview to inform the planning of subsequent interviews. The interviews were continued until data saturation was achieved, which is indicated by the absence of new categories and the saturation of existing categories based on their characteristics and dimensions30,31. The interview data underwent conventional content analysis. In the first step each text was reviewed for immersion and acquiring insights and deep understanding around the phenomenon under study. In step 2 meaning units were determined based on the objectives and the study questions. In step3 important points were extracted as open codes, considering their clear and hidden meaning units. In step4 these codes were categorized under broader titles based on their similarities and differences, and in step 5 the data analysis continued until the themes were extracted30,31. In order to ensure the trustworthiness of the process, Guba and Lincoln criteria were used32. To enhance the credibility and reliability of the findings, various methods were utilized. These included a comprehensive examination of data sources such as semi-structured interviews, observation and field notes, as well as prolonged engagement with the data. Additionally, member checking and peer checking were employed to validate the extracted concepts and themes. Four participants and two peers were involved in this process, all of whom confirmed that the findings aligned with their own understandings and interpretations. The transferability of the study was ensured through a thorough description of the participants, interviews, and analysis. Furthermore, confirmability was achieved by accurately recording participant narratives and providing a detailed report of the study, facilitating the possibility of follow-up by other researchers. Finally, 1214 codes were which were categorized into twenty five subcategories, eleven categories, and three main themes, which were “moral sensitivity,” moral courage,” and “moral commitment” Fig. 1. During the study phase, there were an equal number of male and female participants, totaling 20 individuals, with an average age of 39.51 ± 2.51 years. Additionally, the majority of participants held a master’s degree in nursing, possessed an average work experience of 12.98 + 1.15 years, and had a monthly income of approximately $550.
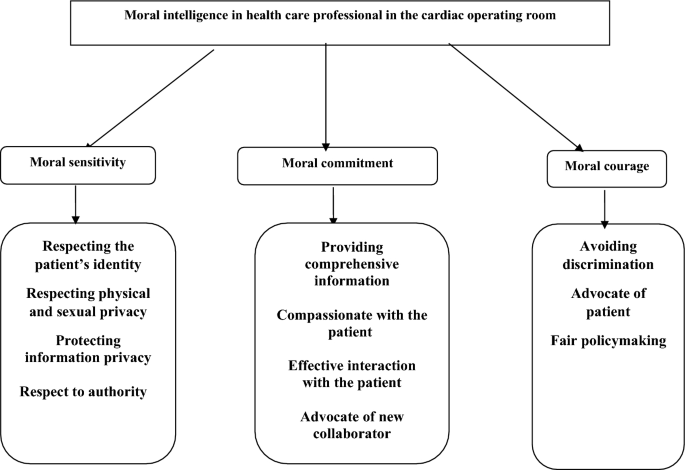
The main themes and subthemes in health care professional’s perceptions.
Phase II. Psychometric properties
Questionnaire development
The assessment scale was created by generating 43 potential items from the qualitative data, which represented the main themes. Furthermore, seven additional items were included based on the findings from the literature review14,21,22,24, resulting in a total of 50 items. Subsequently, the research team evaluated the items and eliminated nine redundant ones, resulting in a final count of 41 items. These items were then categorized into three dimensions: “moral sensitivity” (consisting of 20 items), “moral courage” (comprising 10 items), and “moral commitment ” (comprising 11 items).
Content validity
The content validity assessment involved consulting a panel of experts consisting of 15 professionals, including nurses, operating room nurses, doctors, and surgeons in the heart operating room. This expert panel evaluated the items regarding language, understanding, and suitability to the Iranian culture and context. Based on their evaluation, they suggested removing three items, leaving 38 questions for quantitative analysis of content validity using the content validity ratio (CVR) and content validity index (CVI)33. In order to accomplish this, the panel was given the instrument back, and they were requested to evaluate the items based on their relevance and importance to the study’s subject matter. According to the Lawshe table, the acceptable CVR was reported as 0.4934,35. However, five items with a CVR of 0.33 were removed from the study. The content validity index (CVI) was then evaluated for each remaining item. The revised instrument was given back to the panel, who were asked to rate each item’s relevance, simplicity, and clarity on a four-point Likert scale ranging from 1 to 4. The CVI was calculated for both individual items and the entire instrument. For this study, a CVI value greater than 0.8 was deemed acceptable36. However, three items had a score below this cut-off and were also deleted.
Face validity
The revised instrument with 30 items was then given to 30 healthcare professionals using the same inclusion criteria as for Phase 1. They were asked to assess each item regarding difficulties, relevance, grammar, vocabulary, and intelligibility. The participants declared that the items were simple, clear, and relevant to the study’s topic. In addition, an impact score was calculated in which participants evaluated each item using a five-point Likert scale ranging from one (very little (to five (very much), with a score > 1.5 considered acceptable35. The impact score for all items was higher than 1.5. Therefore, no further items were deleted.
Item analysis
A 30-item instrument was created based on the previous stage. Thirty eligible healthcare professionals used a five-point Likert scale (1 = very low, 2 = low, 3 = to some extent, 4 = high, 5 = very high) to rate themselves on the 30 items. The correlation coefficients between the items ranged from 0.3 to 0.7, and the total score across all items was calculated to be greater than 0.336. All items met these criteria, and it was decided no further items were deleted. Finally, this scale includes ‘“moral sensitivity” (16 items), “moral commitment” (9 items), and moral courage” (5 items).
Participants and data collection
Three hundred healthcare professionals were recruited using a convenience sampling from six public centers providing care to patients in cardiac operating rooms affiliated with medical universities in Iran. The inclusion criteria were having at least 12 months of work experience in the cardiac operating room, being Iranian, having a good command of Farsi, and willingness to participate in the study. The participants’ socio-demographics were also collected. Data were analyzed using descriptive and inferential statistics via the SPSS software, v. 19 (SPSS Inc, Chicago, Illinois, USA). The mean participant’s age was 38.58 ± 2.78, ranging from 26 to 57 years. Most participating in this phase were men (57.33%), married (62.33%), had a bachelor’s degree (52.33%), had about 14.78 + 1.74 years of work experience and an average monthly income equal to 560 US dollars.
Contrast validity (Exploratory factor analysis, convergent validity)
Construct validity helped ensure that the instrument measured what it intended to measure35,36. Exploratory factor analysis using the varimax rotation was used in this study. To achieve the most appropriate structure, eigenvalues higher than 1.0, factor loadings higher than 0.50, and the so-called ‘elbow criterion’ regarding the eigenvalues were considered33,37. The Kaiser–Meyer–Olkin (KMO) and Bartlett’s tests were performed to evaluate sample adequacy. For exploratory factor analysis, the KMO value had to be greater than 0.05. Pearson’s correlation coefficients were calculated between the developed instrument and the the moral comoetence scale for home care nurses scale for convergent validity.
Confirmatory factor analysis
Confirmatory Factor Analysis was carried out utilizing AMOS 22 software, and several indices were employed to evaluate the model’s effectiveness. In order to ascertain the adequacy of the model, it was imperative to adhere to the following stringent criteria: goodness of fit index (GFI) exceeding 0.90, a root mean square error of approximation (RMSEA) below the acceptable threshold of 0.08, a Tucker Lewis Index (TLI) surpassing the minimum acceptable level of 0.90, and a comparative fit index (CFI) exceeding the requisite threshold of 0.90, as per established conventions31,35.
Reliability
To ensure the validity of this instrument, both Cronbach’s alpha coefficient and test–retest reliability analysis were utilized. The internal consistency reliability was evaluated by calculating Cronbach’s alpha coefficient with a sample size of 300 participants. The acceptable Cronbach’s alpha coefficient was determined to be above 0.7. Fortest–retest reliability, the intra-class correlation (ICC) was calculated by collecting data from 70 participants at a two-week interval37.
Ethical approval and consent to participate
Research Center the west of Iran provided ethics approval (IR.UMSHA.REC.1402.538). All methods were performed in accordance with the relevant guidelines and regulations, and all the research methods met the ethical guidelines described in the Declaration of Helsinki. Also, at the beginning of each interview, the researcher introduced herself, explained the study’s goals, and provided assurance that all information would remain confidential and that they could withdraw from the study at any time. They reassured participants that their decision to not participate or withdraw would not have any negative consequences for them. Lastly, the researchers obtained informed and written consent from all study participants.
link





